"Impingement" is a term you hear pretty often in the weight room. When people refer to their shoulder, they are most likely referring to their Gleno-humeral joint. It's where the head of the humerus (upper arm) meets the Glenoid Fossa:

The GH joint is a ball and socket joint, which means it has a capacity to move in large ranges of motion. This would be the opposite of a "hinge joint" such as the knee, which for the most part moves in one plane of motion, with some slight internal and external range of motion capabilities. If you take a look at the picture above, there is a beak shaped structure to the left of the glenoid fossa called the acromion process. Unlike the picture depicts, there is actually an extremely small amount of space between the head of the humerus and the acromion process. In order to raise your arms overhead, the rotator cuff muscles must first depress the head of the humerus to clear some space out to avoid "pinching" of the ligaments and tendons in between the head of the humerus and the acromion. If the rotator cuff isn't strong enough to do so, or there is a lack of stability in your scapulo-thoracic joint (because of poor posture, lack of proper programming in workouts, poor exercise selection, etc.), impingement occurs. There are three types of acromions:

You'll notice that type 1 has more or less a flat surface, type 2 is slightly curved, and type 3 has a pretty sharp hook to it. From this, one can surmise that the type three acromion shortens the space between the head of the humerus the most because of its "beak-like" structure, and therefore, can increase the likelihood of impingement syndrome. Your acromion can actually "morph" from a type 1 or 2 into a type 3. This change can occur from poor posture and a poor training program, which I'll go over in more detail later on. I'm more of a believer of contraindicated people, rather than contraindicated exercises; however, the majority of people I see at the gym tend to have poor posture, as well as poor training programs. This is why I included upright rows, and bench dips as "contraindicated exercises" in my first post.
Unfortunately, I can't change the shape of your acromion. But in this post, I'll show you how to improve your posture, strengthen your scapular stabilizers, and provide proper balance in your workouts.
1) Thoracic Spine Mobility. I explained in my last couple of posts how an immobile T-Spine leads to a more mobile lumbar spine, which is exactly what we do not want. Along those same lines, an immobile T-spine will lead to a more mobile scapulo-thoracic joint (ST). In my post A Joint-by-Joint Approach to Training, I went over that we want a stable ST joint, and a mobile GH joint. Our scapulae (shoulder blades) can tilt anteriorly and posteriorly. When we raise our arms overhead, our scapulae should tilt posteriorly to allow the movement to occur. But, let's say our t-spine isn't mobile enough for it to tilt properly:

Round your shoulders forward and poke your chin out like this desk jockey above. Now, in that same position, try to raise your arms up overhead. Your body will not allow it. This will kind of give you an idea of how a person with poor t-spine mobility will lead to poor scapular stability as well as shoulder mobility. My last post shows you some videos on how to improve mobility in your upper back.
2) Scapular Stability. The average gym-goer will not know what the heck a serratus anterior or where their lower trapezius is located. These two muscles perform a crucial role in stabilizing the scapula when raising your arms overhead. Individually, the serratus anterior protracts (pushes forward) the scapula, the lower trapezius depresses the scapula, and the the upper trapezius elevates the scapula. Collectively, they make up the "force couple" to help rotate the scapula to move the arms overhead:
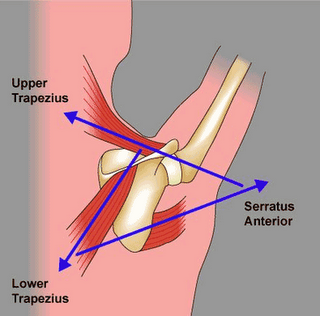
Most people have very overactive upper traps and an underactive serratus anterior and lower trap. So how do we activate and strengthen these two neglected muscles?
Serratus Anterior: Hand Switches
Keep your core tight - you do not want your hips to sag. Just walk with your hands back and forth. Do 3 sets of 30 seconds each. Going as quickly as you can while maintaining proper form.
Lower traps: Wall Slides
Make sure you squeeze your shoulder blades together, keep your butt on the wall, and keep your shoulder blades down. When your elbows reach the bottom position, try to squeeze both elbows down and towards each other. If you do it right, you should feel it in the middle of your back. Do 3 sets of 12 reps.
3) Pull more than you push!
We need to strengthen our back muscles in order to maintain optimal postural alignment. If you go to the gym and do only pushups and bench presses, you're only reinforcing poor posture and effectively shortening your internal rotators so that you look like the desk jockey I showed you above. The cable row machine is one of the few machines I actually like. It's very hard to train the scapular retractors without cheating or compromising your lower back. We've all seen these meatheads at the gym:
The cable row allows you to stay upright and use an appreciable load, while maintaining good form.
Rotator cuff exercises are extremely overrated. Truth of the matter is, if you lack t-spine mobility, extra 'cuff work will be of little or no use to you. If you have the first three components of a balanced training program in check, then some external rotations will definitely help out, but don't think it is the cornerstone of your workout.
Train Hard,
Jason
Great post. I am a physical therapist and love the advice given here. So many people ignore posture when it comes to exercise and avoiding pain and injury. Keep up the grat advice.
ReplyDelete~JTrempe PT, ATC
http://www.joint-pain-solutions.com